
More Information
Submitted: February 25, 2025 | Approved: March 03, 2025 | Published: March 04, 2025
How to cite this article: Sauerheber R. Fluoridation Story Essentials, 1939 to 2025. Arch Case Rep. 2025; 9(3): 077-080. Available from:
https://dx.doi.org/10.29328/journal.acr.1001131
DOI: 10.29328/journal.acr.1001131
Copyright license: © 2025 Sauerheber R. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Drinking water fluoridation; Fluoride chemistry; Fluoride toxicity; Fluoride ingestion

Fluoridation Story Essentials, 1939 to 2025
Richard Sauerheber*
Palomar Community College, 1140 W. Mission Rd., San Marcos, CA 92069, USA
*Address for Correspondence: Richard Sauerheber, Palomar Community College, 1140 W. Mission Rd., San Marcos, CA 92069, USA, Email: [email protected]
The history of the use of industrial fluoride compounds infused into drinking water is briefly summarized. The lack of oversight by Federal regulatory agencies conflicts with its recommendation by the Oral Health Division of the Centers for Disease Control. The chemistry of fluorides is discussed along with the toxic effects of fluoride ingestion. The U.S. Food and Drug Administration has never approved fluoride for ingestion and has instead ruled that it is unsafe to add to foods and prohibits the sale of fluoride compounds intended for ingestion by pregnant women. Legal issues are introduced. The appearance of severely fluorotic and normal leg bones is shown.
In 1939, the Nazi Army invaded Poland to start World War II Coincidentally that same year, the National Institutes of Health director Trendley Dean published that unsightly dental fluorosis might actually be desirable by decreasing the incidence of tooth decay [1]. Unfortunately, only a limited data set from a few Midwestern towns was used to reach that conclusion. We now know that when all data are examined, there is no significant decrease in dental caries from consuming water containing natural calcium fluoride, even as high as 6 parts per million (ppm) [2]. Moreover, today dental fluorosis is known as enamel hypoplasia, the first visible sign of poisoning from fluoride ingestion [1-3].
Sodium fluoride is necessary to make uranium hexafluoride needed for bomb-grade uranium enrichment. In 1945, two nuclear bombs were dropped on Japan to finish the war in the Pacific. In January of that year, the Public Health Service and the U.S. Surgeon General ordered the infusion, into public drinking water, of sodium fluoride stockpiled from the nuclear bomb industry [1]. Without regard for the vastly lower solubility and toxicity of calcium fluoride (CaF2)[4], the fluoride level to use from sodium fluoride (NaF) was settled at 1 ppm, where teeth enamel fluorosis had been considered to be not too severe from natural water. The chosen city for the test was Grand Rapids, Michigan, the first city to be provided drinking water treated with industrial sodium fluoride [1], now in 2025 fluoridated for almost an average U.S. human lifespan. Although this is considered by many to be a conspiracy, the actions are truly believed by modern proponents to help prevent dental caries in children.
Sadly, the experiment that was to be monitored for 10 years was not, since officials interpreted missing teeth as the absence of cavities, where it is now known that systemic fluoride can abnormally delay teeth eruption. Since no obvious adverse health effects were noticed by the officials, artificial “fluoridation” was presumed to be a successful public health procedure by the then Public Health Service [1,3].
The U.S. Food and Drug Administration has never approved any fluoride compound for ingestion, ruled in 1975 that fluoride is considered unsafe to add to foods, its addition into public drinking water is an uncontrolled use of an unapproved drug, and in 1966 prohibited the sale of any fluoride compound intended to be ingested by pregnant women [4,5]. No objection however was officially raised by government officials when fluoridation first began in 1945, to avoid any possible interference with the war effort [1]. By the 1960s, under the robust encouragement of the Centers for Disease Control and U.S. Surgeons General, most major U.S. cities were treating citizens with industrial sodium fluoride, not natural calcium fluoride for which the original observation was made.
The fluoride ion from industrial compounds is a toxic calcium chelator. This includes sodium fluoride used in toothpaste and dental gels, and fluosilicic acid (H2SiF6) used for water “fluoridation” since 1985 when the director of the Environmental Protection Agency Rebecca Hanmer decided that this fertilizer industry hazardous waste could be substituted for sodium fluoride as a convenient way to dispose of it [4].
Unfortunately, ingested fluoride from water that lacks high levels of calcium is converted into the corrosive hydrofluoric acid HF in the acidic stomach. HF as a neutral small molecule gains entry into the alkaline bloodstream where it dissociates into fluoride ions again [4]. As a calcium chelator, blood fluoride binds to normal bone hydroxyapatite, converting bone to abnormal hydroxyapatite, which is less soluble than normal bone [2], in a process that begins with the first sip of fluoridated water and accumulates during lifelong continuous consumption. Normal and severely fluoridated tibia and fibula bones are pictured (Figure 1).
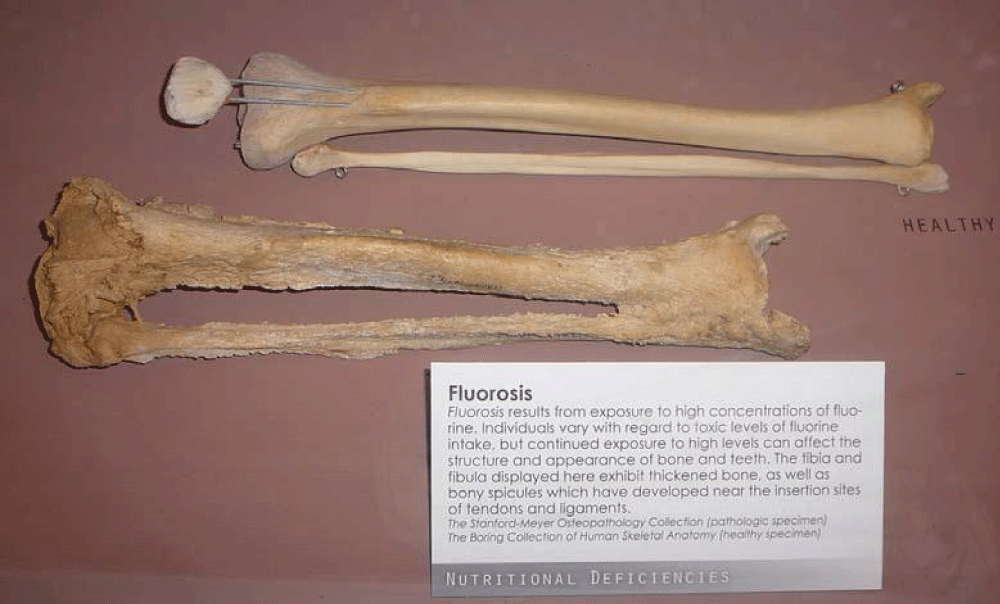
Figure 1: Normal tibia and fibula human leg bones are pictured (top) along with tibia and fibular human leg bones from an individual afflicted with severe skeletal fluorosis. The conversion of normal bone into abnormal fluorapatite begins with the first sip of fluoridated water, where 95% of all retained ingested fluoride resides permanently in bone. The diseased tibia and fibula bones here at about 12,000 mg/kg fluoride required a long period of subacute fluoride level exposure to produce bone thickened and spiculed to this extent. A Stage III level of destruction with bone pain at about 6,000 mg/kg fluoride from 0.7 ppm fluoridated water alone would require an estimated 70 years of continuous consumption.
Acute poisoning from synthetic fluoride ingestion is not rare. At blood levels of ~3 ppm, death is from heart block due to the fluoride interference of calcium mobility, where extracellular calcium is the mediator between electrical excitation and contraction of heart muscle cells. Accidental fluoridation overfeeds have occurred, and in Hooper Bay, Alaska, 302 people were severely poisoned with acute stomach and chest pain, with one fatality [4].
Chronic poisoning from heart failure due to fluoride-induced muscle degeneration occurs at a blood fluoride level of 1ppm. The use of 1 ppm fluoridated water in kidney dialysis wards was prohibited by the FDA due to the high incidence of mortality of dialysis patients treated with such water which must now be de-fluoridated for this purpose [4].
Most consumers of fluoridated water had blood fluoride levels at about 0.1 ppm until 2011 when the U.S. Health and Human Services lowered the allowed water level to 0.7 ppm in an attempt to reduce rampant dental fluorosis in U.S. teenagers. The blood level is now estimated at 0.07 ppm for those who faithfully consume treated drinking water. At such “low” levels that are not considered acutely toxic, bone fluoride accumulates to thousands of mg/kg over decades of time and causes progressive bone weakening leading to bone pain often considered to be arthritis, at an estimated 2-4,000 mg/kg [2]. Fluoride is the only toxic substance that pathologically causes parathyroid hormone and calcitonin blood levels to both increase at the same time [2]. This is because fluoridated bone is less soluble for resorption by PTH to prevent low blood calcium levels to protect the beating heart, while paradoxically at the same time, calcitonin increases bone formation from blood calcium to attempt to restore normal bone to replace fluoridated bone.
Fluoride crosses the blood-brain barrier and also the placental-fetal membrane. Children born to pregnant women who consume fluoridated water have increased risk of lowered IQ [2,6]. Use of fluoridated water during bottle feeding increases the risk of dental fluorosis. In fact, not surprisingly, all fluoridated cities have increased incidence of dental fluorosis, without exception [4]. The magnitude of these effects always depends on the calcium content of the water since calcium mitigates the assimilation of ingested fluoride. It must be noted that infant mortality is highest in those fluoridated U.S. States that have soft calcium-deficient water supplies [7].
The EPA allows water fluoridation because it is intentionally added to treat teeth as though it somehow were an effective decay preventive dentifrice, and is not an accidental spilled pollutant. Ironically, the Safe Drinking Water Act was originally written to prevent the spread of water fluoridation in the U.S. [8], stating that no National requirement can be made to add any substance into water other than to sanitize water and that States can be no less restrictive. This is why the CDC only “recommends” fluoridation and does not require it.
An FDA petition to ban water fluoridation was reviewed for eight years [5], leading to the conclusion that fluoride is toxic at any concentration and that the EPA must regulate its addition into water under the Toxic Substances Control Act (TSCA). The EPA Office of Water wrote however that the FDA must regulate fluoridation because it is added to treat humans.
The Federal District Court, San Francisco trial that requests a ban on water fluoridation, because it violates the TSCA, led Judge Chen to rule that the EPA must address the fact that current fluoride levels in U.S. treated water supplies are an unreasonable risk to human health [6]. The TSCA however categorically prohibits adding any toxic substance into public water supplies at any concentration (other than to sanitize water) [4,5]. The EPA argues that the adverse health effects from fluoride ingestion are not the fault of water fluoridation, but rather other fluoride sources. However, fluoride from drinking water in fluoridated cities is responsible for 65% of the total fluoride in the bloodstream of such city populations [3].
The CDC published in 2001 that systemic blood fluoride does not reduce dental decay [1,2,4] but this has not caused the Agency to halt fluoridation and prompted its Oral Health Division to claim that the drinking water effect must therefore be topical. But CDC officials were asked in writing how salivary fluoride from blood during ingestion of 1 ppm fluoridated water that bathes teeth at only 0.006 ppm [3], 250,000 times less concentrated than in toothpaste, or fluoridated water at 0.7 ppm, 2,142 times less concentrated, can reduce dental decay topically. CDC officials wrote that an answer would be provided, but have never answered this question after many years.
The recently appointed Health and Human Services head Robert F. Kennedy, Jr. is vocally opposed to fluoridation of water and issued an order for the CDC to recommend, but not require, that the procedure be halted. However, his long stance denouncing most vaccines and other positions may minimize the effectiveness of the request to halt fluoridation and in fact has caused intense opposition. Incredibly, after the ruling by Judge Chen, some officials reacted by stating that it is acceptable to have a slight IQ deficit as long as dental caries are prevented. RFK correctly states that governments should not decide what substances the public must drink. But in two court trials that proved fluoridated water increases incidence of cancer lethality [4,8], the rulings were overturned ironically with that very argument, that courts should not determine what people should drink. Although the FDA and EPA are jointly delinquent by not banning fluoridation, decimating these Agencies would cause all the good the Agencies do to disappear. Since the Federal court trial, as of this date, over 54 cities have now halted fluoridation and the State of Utah has formally banned it.
Fluoride ion is present naturally in the oceans at 1 ppm, but the extremely high calcium levels minimize its assimilation after ingestion. Pristine fresh water does not contain fluoride, while some sources are naturally contaminated with calcium fluoride that is always also accompanied with protective calcium from other salts. If the only fresh water source available to drink is fluoridated, then it is necessary to drink it to remain hydrated. But to minimize further accumulation in bone and other effects, it needs to be avoided from one’s diet. Not using fluoride toothpaste and only drinking non-fluoridated water will reduce the blood fluoride level by 80% [3]. Fluoride from toothpaste or gels does not incorporate into the enamel matrix anyway. Tooth enamel is a derivative of bone, but unlike bone is a hardened crystalline hydroxyapatite form. Topical fluoride forms precipitates on teeth surfaces with salivary calcium [4] which are readily washed away on eating or drinking, to be swallowed. The idea that fluoride “remineralizes” teeth enamel is incorrect since normal enamel consists of hydroxyapatite, a hydrate of calcium phosphate (Ca5(PO4)3(OH).
The spherical fluoride ion is similar in size to a water molecule which makes it difficult to filter from water. Modern reverse osmosis units (from Costco or the GE Profile) have pore sizes that under pressure produce de-fluoridated water. One can also purchase distilled water, or use a distiller such as from Ohio Distillers that collects evaporate and leaves fluoride contamination behind. It is recommended to add minerals or lemon juice prior to consumption. Bottled water can be purchased if it has been reverse osmosis treated or is from a natural spring with low fluoride. Arrowhead water however wrote that it distributes water from various sources and has a wide range of fluoride levels up to 1.2 ppm. Fluoride can be removed by ion exchange, but this is expensive and requires regular maintenance and media replacement. Typically marketed fluoride filters are aluminum oxide based and cannot be sold in alkaline water regions since hydroxide binds aluminum more readily than fluoride does. These bind fluoride for a short time and the possibility of aluminum leakage into product water has not been disproven. Bone char from Scotland (not Argentina as this author tested) can bind fluoride, but sources of char have become more scarce and can leave a residual taste in the water.
The incidence of dental caries has been declining in countries around the world regardless of fluoridation status ever since the widespread availability of toothbrushes and toothpaste, where caries are caused by the dissolution of enamel hydroxyapatite by acid-producing bacteria. It is most unfortunate that an association made over 80 years among limited data has caused the notion to spread that fluoride ingestion might substantially reduce teeth decay. This has been thoroughly disproven. and the adverse effects of systemic fluoride causing irreversible dental fluorosis poisoning, fluorosis of the bony skeleton that is not reversed by transfer to non-fluoridated water, and adverse effects on brain development at quite low concentrations are well documented. Federal regulatory agencies and water legislation have provided some benefit in controlling fluoridation of water supplies and people, but have been ineffective in halting the harmful practice. Consumers are advised to avoid ingestion of fluoride added into drinking water and dental products as much as possible since the ion is not a normal component of human blood, is not a mineral nutrient [9], and in fact fluoride from soluble compounds used in water fluoridation is a recognized toxic calcium chelator [ref. 16 in 4].
Disclaimer: This material here does not necessarily represent the views of Palomar College or its staff.
- Bryson C. The Fluoride Deception. N.Y.: Seven Stories Press. 2006.
- Connett P, Beck J, Micklem HS. The Case against Fluoride: How Toxic Waste ended up in Our Drinking Water and the Bad Science and Politics that keep it there. USA: Chelsea Green Publishing. 2010.
- National Research Council. Fluoride in Drinking Water: A Scientific Review of EPA’s Standards. Washington, D.C.: The National Academies Press. 2007.
- Sauerheber R. Physiologic conditions affect the toxicity of ingested industrial fluoride (as used in water fluoridation). J Environ Public Health. 2013;439490. Available from: https://doi.org/10.1155/2013/439490
- U. S. Food and Drug Administration. Dockets Management, Petition FDA-2007-P-0346. Petition for reconsideration, non-personal supplements as appropriate, not for sale but for dissemination of information for public benefit. 2007. Available from: http://www.regulations.gov/#!searchResults,rpp=25,po=0,s=FDA%252B2007-P-0346,fp=true,dct=FR%252BPR%252BN%25
- United States District Court, Northern District of California. Food and Water Watch vs. EPA, Case 3:17-cv-02162-EMC, Document 445, Filed 09/24/24. Available from: https://www.cand.uscourts.gov/wp-content/uploads/2024/09/17-cv-2162-Food-_-Water-Watch-Inc.-et-al.-v.-EPA-et-al-Opinion.pdf
- Sauerheber R. High infant mortality and morbidity in fluoridated soft water U.S. states. J Environ Toxicol Anal Res. 2023;4:1-15. Available from: https://www.scholarena.com/article/High-Infant-Mortality-and-Morbidityy.pdf
- Graham JR, Morin P. Highlights in North American litigation during the twentieth century of artificial fluoridation of public water supplies. 1999. Available from: https://law.fsu.edu/sites/g/files/upcbnu1581/files/JLUEL/jluel-v14n2.pdf
- Peckham, S and Awofeso, N., Water Fluoridation: A Critical Review of the Physiological Effects of Ingested Fluoride as a Public Health Intervention, The Scientific World Journal, 2014. http://dx.doi.org/10.1155/2014/293019